

Abstract
Background: Bortezomib is a proteasome inhibitor that can lead to cell-cycle arrest and apoptosis. Bortezomib-based regimens are widely used as induction therapy of multiple myeloma (MM). Unlike lenalidomide (an immunomodulatory drug), the role of bortezomib in the consolidation and maintenance therapy of multiple myeloma is less clear. This study aims to examine the efficacy and safety of bortezomib-based regimens as consolidation/maintenance therapy in MM patients following induction therapy with or without autologous stem cell transplantation (ASCT).
Methods: PubMed, ASH, and ASCO databases were searched for randomized controlled trials (RTC) of bortezomib-based regimens (either single-agent or combination) as consolidation/maintenance therapy for MM patients through July 2018. Study endpoints included overall survival (OS), progression-free survival (PFS), and adverse events (AE). Pooled hazard ratios (HR) for survival outcomes and relative risks (RR) for dichotomous data with 95% confidence interval (CI) were calculated with a random effect model using MedCalc (MedCalc Software, Ostend, Belgium). For studies that did not report HRs for survival outcomes but provided graphical survival curves, the log HRs and variances were estimated based on the method by Parmar et al (Stat Med 1998; 17: 2815-2834). Heterogeneity was assessed using the I2 statistic of inconsistency, with statistically significant heterogeneity defined as I2 > 50% or p-value < 0.1.
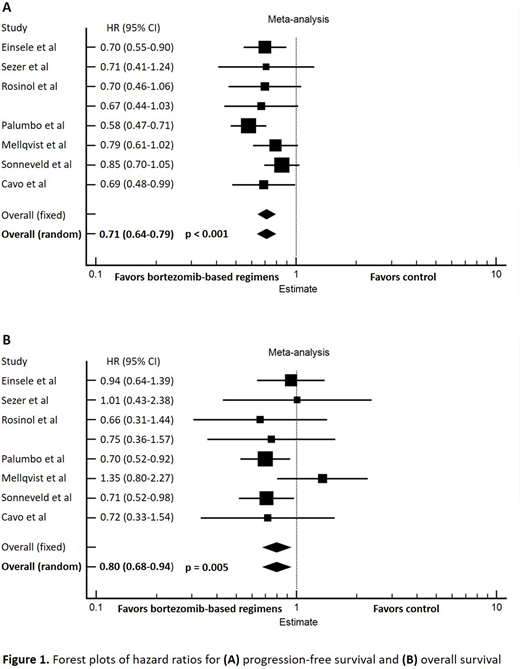
Results: Eight randomized controlled trials (7 phase III, 1 phase II; 2 were published in a single article) were identified. Bortezomib-based regimens were administered as consolidation treatment in 5 RTCs and maintenance therapy in 3 RTCs, following induction therapy +/- ASCT. A total of 2439 patients were included: 1154 patients received bortezomib-based regimens, and 1285 patients received non-bortezomib-based regimens or observation. Two RCTs (1 for consolidation, 1 for maintenance) did not provide HRs, which were estimated as described as above. Pooled data from the 8 RCTs showed that bortezomib-based consolidation/maintenance therapy improved progression-free survival (HR 0.71, 95% CI 0.64-0.79, P < 0.001; I2 = 6.61%) and overall survival (HR 0.80, 95% CI 0.68-0.94, P = 0.005; I2 = 0%) compared to observation or regimens without bortezomib. When the 2 RCTs that did not report HRs were excluded from the meta-analysis, it did not alter the favorable outcome of bortezomib-based consolidation/maintenance therapy: PFS (HR 0.70, 95% CI 0.60-0.82, P < 0.001; I2 = 40.54%) and OS (HR 0.76, 95% CI 0.64-0.91, P = 0.002; I2 = 0%). The PFS benefit was maintained in a subgroup analysis by the setting of treatment (consolidation, HR 0.73, 95% CI 0.63-0.85, P < 0.001; I2 = 0%, maintenance, HR 0.70, 95% CI 0.56-0.0.86, P = 0.001; I2 = 55.63%). Bortezomib-based therapy prolonged OS in the maintenance setting (HR 0.71, 95% CI 0.58-0.86, P < 0.001; I2 = 0%) but not in the consolidation setting (HR 1.01, 95% CI 0.77-1.33, P = 0.935; I2 = 0%). Regarding safety, bortezomib-based consolidation/maintenance therapy significantly increased the risk of grade 3 or 4 peripheral sensory neuropathy and neuralgia (RR 2.09, 95% CI 1.11-3.95, p = 0.022; I2 = 52.64%) compared to observation or regimens without bortezomib. There was a trend toward increased rates of grade 3 or 4 thrombocytopenia (RR 1.54, 95% CI 0.95-2.52, p = 0.08; I2 = 21.67%), GI symptoms (RR 2.54, 95% CI 0.63-10.25, p = 0.19; I2 = 76.72%), vascular events (RR 1.90, 95% CI 0.80-4.53, p = 0.15; I2 = 0.00%), and fatigue (RR 2.10, 95% CI 0.83-5.30, p = 0.12; I2 = 0.00%) with bortezomib-based consolidation/maintenance, but these did not reach statistical significance.
Conclusions: Bortezomib-based consolidation/maintenance significantly improves PFS and OS in MM patients following induction therapy +/- ASCT. The OS benefit appears to be limited to the maintenance setting based on a subgroup analysis. Bortezomib-based regimen increases the risk of grade 3 or 4 peripheral sensory neuropathy and neuralgia.
Bachanova:Gamida Cell: Research Funding; GT Biopharma: Research Funding; Kite Pharma: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal